Seizure Disorder
Seizure Disorder
Course Description
This course covers the detailed description of seizure disorder, its risk factors, manifestations, investigations, management strategies and prevention.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- Definition and brief introduction to seizures or epilepsy
- Risk factors contributing to epilepsy or seizures
- Pathogenesis of seizures
- Manifestations of epilepsy
- Laboratory Tests and Imaging
- Differential Diagnosis
- Treatment/Management
- Prognosis
- Economic impact of the disease
- Prevention
Course Content
COURSE DESCRIPTION
Seizure disorder or epilepsy is a heterogeneous group of disorders, which involve abnormal neuronal activity producing abnormal sensations, convulsions or muscle spasms. Seizure disorders affect 2.2 million people in United States, which impose a significant burden on the National economy. This course covers the detailed description of seizure disorder, its risk factors, manifestations, investigations, management strategies and prevention. The course will empower the knowledge of medical professionals especially the nursing students regarding seizure disorder. Updating knowledge about seizure disorder would make the healthcare professionals capable of dealing the patients suffering from seizures with ease and confident.
INTRODUCTION
Seizure disorder or epilepsy is a heterogeneous group of disorders, which involve abnormal neuronal activity producing abnormal sensations, convulsions, muscle spasms or even disagreeable changes in emotions (Bromfield, et al. 2006). Epilepsy is defined as “any disorder characterized by recurrent unprovoked seizures” (Papadakis & McPhee, 2015). For the way of explanation, seizures refer to the sudden uncontrolled activity of brain that may manifest in the form of convulsions, minute physical changes, disturbed thoughts and unpleasant emotional changes. Epilepsy has significant psychosocial consequences and affects individual’s quality of life severely. Most importantly, illness-related stigma has powerful effects on psychosocial wellbeing, routine life and overall health of the patient.
Risk factors of seizures or epilepsy include family history of epilepsy (genetics), perinatal injuries, history of head trauma, metabolic abnormalities, tumours in brain, vascular diseases and infectious diseases (Papadakis & McPhee, 2015). Seizures can be focal as well as generalized. Unprovoked seizures usually have prodromal symptoms such as headache, mood changes, malaise and myoclonic jerks. In order to prevent further attacks of seizures, the patients with epilepsy are treated with antiepileptic drugs depending on the type of seizures, until they are seizure-free for at least the period of two years (Papadakis & McPhee, 2015).
Epilepsy imposes significant burden on the country’s income. It affects 2.2 million in United States and 50 million people all over the world (Santhosh, et al. 2014). In terms of disability-adjusted life year (DALY), the estimated burden of epilepsy accounts for 1% of total disease burden globally (Jain, et al. 2008). According to the study on Global Burden of Disease, epilepsy accounts for 9.9% of the combined burden of neurologic and cerebrovascular diseases (Murray, et al. 2010). It signifies that epilepsy imposes extraordinary burden on the quality of life. Therefore, proper evaluation and optimal management of this disorder is critical to reduce its burden and to improve the quality of life.

Figure 1: Seizures (Source: www.blogs.allizhealth.com)
ETIOLOGY AND RISK FACTORS
International League Against Epilepsy classifies etiologies of epilepsy in three groups:
-
Genetic epilepsy
-
Structural or Metabolic epilepsy
-
Unknown
Genetic Epilepsy
Genetic epilepsy includes a large number of disorders, which affect people from neonatal period to adolescence, and even later in life. Most of these disorders follow autosomal dominant pattern of inheritance with mutations in the genes that encodes a neuronal ion channel (Papadakis & McPhee, 2015). Genetic epilepsy may involve voltage-gated potassium, sodium, chloride and calcium channels as well as nicotinic acetylcholine receptors and γ-aminobutyric acid (GABA) receptors (George, 2004).
Structural/Metabolic Epilepsy
A number of causes provoke recurrent seizures.
Pediatric age group – In infancy and childhood, congenital abnormalities and perinatal injuries may cause seizures.
Metabolic disorders – Metabolic disorder such as uremia, hypoglycemia or hyperglycemia may cause seizures. Drug withdrawal is a common cause of recurrent seizures. Being readily reversible causes, these cannot be included in epilepsy.
Trauma – It is an important cause of seizures especially in young age. Most likely, post-traumatic epilepsy occurs when dura mater is injured. Usually, post-traumatic epilepsy occurs within two years of head injury and fits within a week of head injury do not imply that the seizures will occur in later life.
Tumours and space occupying lesions – Brain tumours may lead to seizures at any age. Most often, seizures are the initial symptom in the patients with brain tumour. The tumours of frontal, parietal and temporal regions usually present with seizures. Therefore, the patients presenting with seizures after the age of 30 should be ruled-out for brain tumours (Papadakis & McPhee, 2015).
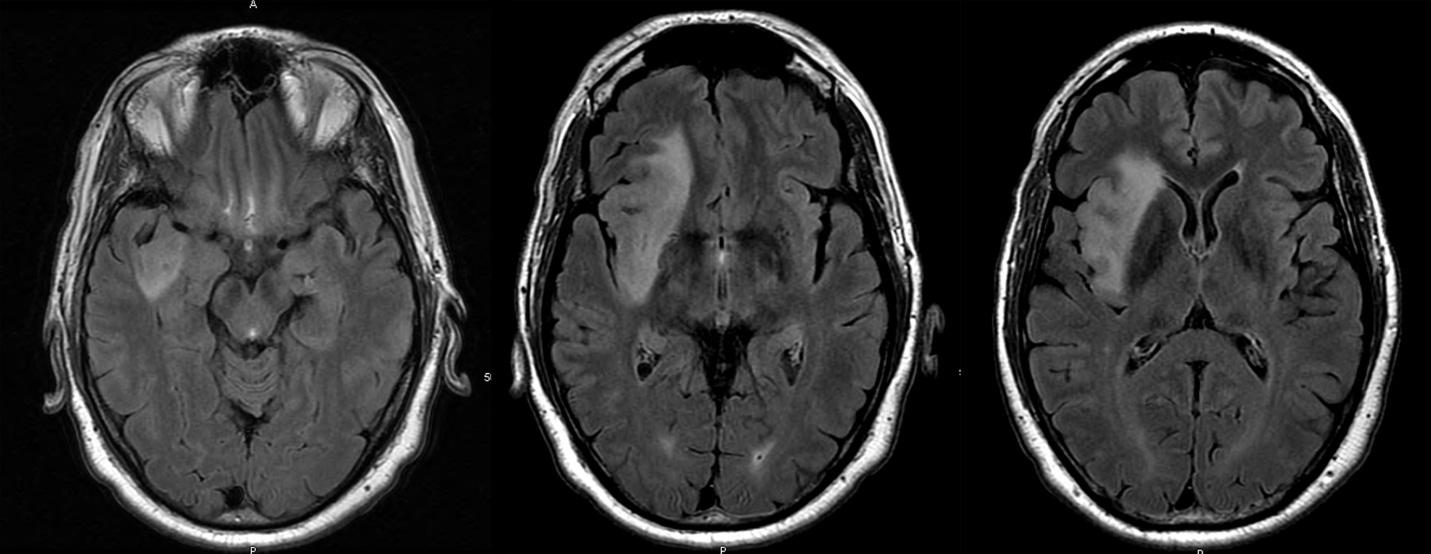
Figure 2: MRI detected right insular tumour in an old patient with history of epilepsy (Source: www.intechopen.com)
Vascular diseases – With the advancing age, vascular diseases cause seizures especially after 60 years of age. Cerebral infarction is one of the common vascular diseases, which cause epilepsy.
Degenerative disorders – Alzheimer’s disease and other degenerating diseases cause epilepsy in older age.
Infectious diseases – Infectious diseases should be considered in those presenting with seizure at any age. Bacterial meningitis, viral encephalitis, neurosyphilis and cerebral cysticercosis may present with seizures. In the patients with AIDS, CNS toxoplasmosis, cryptococcal meningitis and secondary viral encephalitis may cause seizures.
Unknown Causes
In various situations, cause of seizures goes undetected.
CLASSIFICATION OF SEIZURES
Seizures are classified in focal and generalized seizures.
Focal/Partial Seizures
Focal or partial seizures involve only a part of cerebral cortex. The manifestations of focal seizures depend on the area of the brain involved. Focal seizures may alter consciousness and may evolve to convulsive seizures.
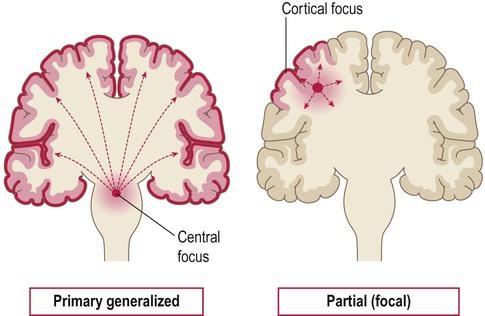
Figure 3: Focal and generalized seizures (Source: www.clinicalgate.com)
Focal seizures without involvement of consciousness – Such focal seizures do not involve altered level of consciousness. Convulsive jerking, paresthesias or tingling sensations spread to the limbs or body parts corresponding to the part of cortex involved. Lesion of visual, auditory, olfactory of gustatory areas in brain may cause special sensory symptoms such as light flashes or buzzing. Additionally, autonomic signs and symptoms such as dilated pupils, sweating, flushing may be the manifestation of focal seizures. Sometimes, dysphasia, illusions, hallucinations or impaired memory may be the only manifestation of the seizures (Papadakis & McPhee, 2015). Previous these types of seizures were called as “simple partial seizures”.
Focal seizures with impairment of consciousness – Such seizures involve altered level of consciousness. Various symptoms such as convulsive jerking, tingling sensations, visual, auditory or gustatory manifestations followed by impaired consciousness or responsiveness. Previously, these types of seizures were named as “complex partial seizures”.
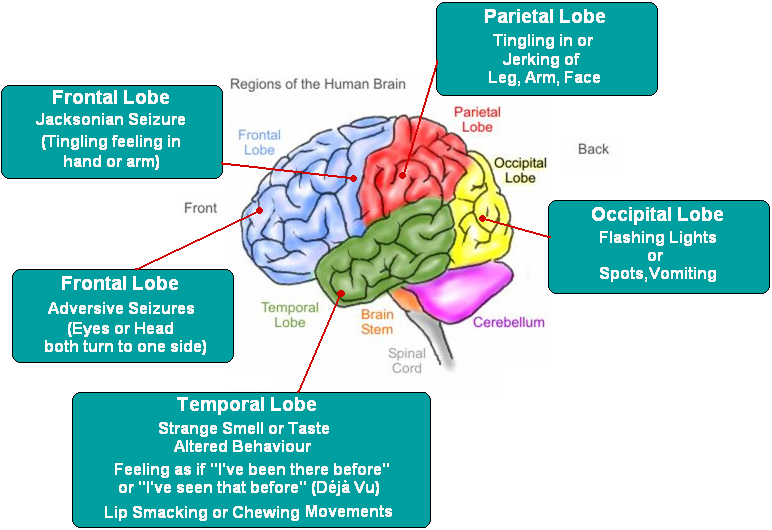
Figure 4: Epilepsy facts in terms of brain regions (Source: www.images.search.yahoo.com)
Generalized Seizures
Generalized seizures involve both the cerebral hemispheres. Such seizures manifest in both sides of the body and always involve brief or long-term alteration in consciousness or responsiveness. Generalized seizures are divided into several categories and, sometimes, the seizures cannot be classified due to lack of information:
-
Absence seizures
-
Atypical absence seizures
-
Myoclonic seizures
-
Tonic-clonic seizures
-
Tonic, clonic or atonic seizures
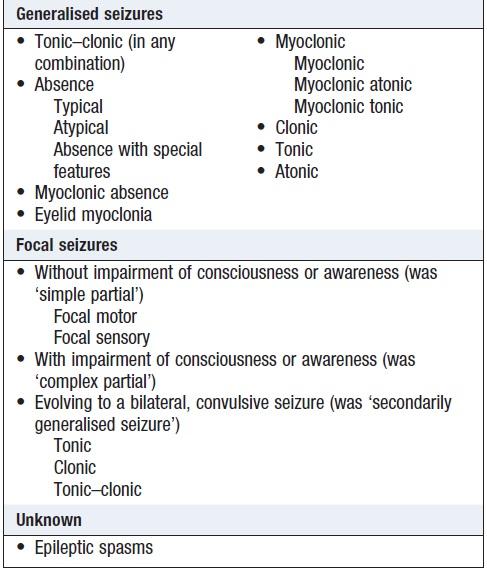
Figure 5: Classifications of seizures (Walker, et al. 2014)
Absence seizures – These types of seizures are characterized by impaired consciousness which may accompany clonic, tonic or atonic components, as well as autonomic symptoms such as enuresis. Absence seizures almost always start in childhood and seize until 20th birthday or change into another form of epilepsy. The onset and termination of absence seizures is abrupt and the patient may experience attacks during conversation missing a few words or impairment of external awareness. Electroencephalography (EEG) shows bilateral bursts of symmetric 3-Hz spike-and-wave activity (Papadakis & McPhee, 2015). The patients with normal EEG and intelligence have good prognosis.
Atypical absence seizures – These seizures have more marked tone and gradual onset as compared to those of typical absence seizures. Such seizures are associated with developmental delay and slower spike-wave discharges.
Myoclonic seizures – These seizures manifest as single of multiple myoclonic jerks.
Tonic-clonic seizures – These seizures are characterized by tonic and clonic phases. In tonic phase, the patient develops sudden loss of consciousness, becomes rigid, falls to the ground, and stops breathing. The tonic phase lasts for less than one minute. Tnoic phase is followed by clonic phase. In clonic phase, the patient jerks body musculature, which lasts for 2-3 minutes. Clonic phase is followed by a stage of flaccid paralysis. The patient may bite his/her tongue or lips, pass urine or stool or may be injured during the attack. The patient may regain consciousness and drift into sleep or remains unconscious and have further attacks (status epilepticus) or regain conscious and have further attacks (serial seizures). Similarly, the patient may behave in an abnormal way after the seizure and remains confused and unaware of the events. This situation is termed as “postepileptic automatism”. Moreover, headache, confusion, drowsiness, muscle pain or combination of these symptoms may be observed in postictal state.
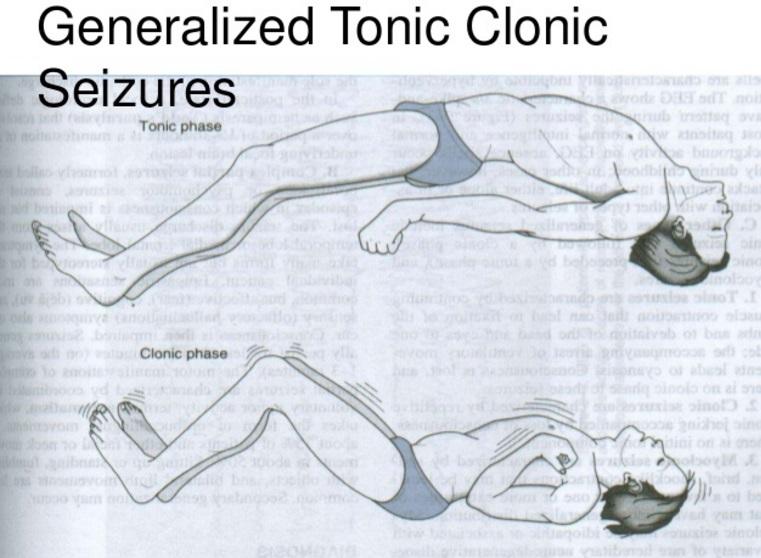
Figure 6: Tonic-clonic seizures - illustration of tonic and clonic phases (Source: www.slideshare.net)
Tonic, clonic or atonic seizures – In these seizures, altered level of consciousness occurs with either tonic or clonic phases. Such type of seizures usually occur in children. Atonic seizures may also be observed. Atonic seizures are also called epileptic drop attacks.
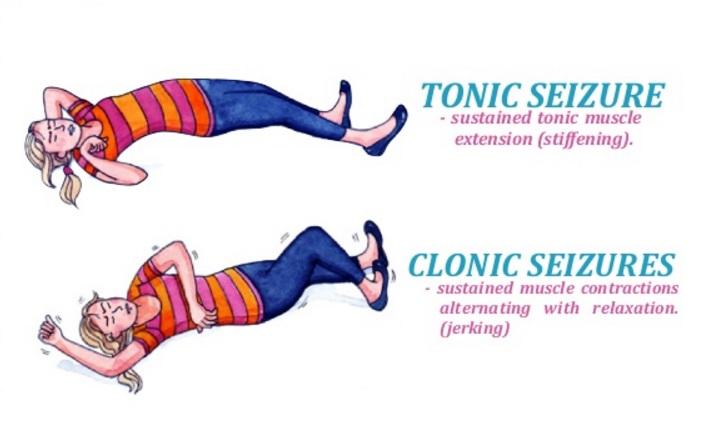
Figure 7: Tonic and clonic seizures (Source: www.slideshare.net)
Figure 8: Atonic seizures (Source: www.epainassist.com)
CLINICAL FINDINGS
Clinical findings of seizures or epilepsy include:
-
Signs and symptoms
-
Imaging
-
Laboratory and other studies
-
Signs and Symptoms
Prodromal symptoms such as headache, mood changes, malaise and myoclonic jerks may alert the patient of impending seizure. Prodromal symptoms are different from aura as aura itself is the part of seizure. The seizures may occur unpredictably irrespective of time or activity. Occasionally, seizures occur at particular time e.g. during sleep. However, there are some situations which may precipitate seizures. These situations include:
-
Lack of sleep
-
Missed meals
-
Emotional stress
-
Menstruation
-
Use of certain drugs
-
Alcohol ingestion or withdrawal
-
Fever
-
Non-specific infections
-
Flashing lights
-
Flickering television
-
Music
-
Reading
Immediately after the seizure, extensor plantar response is observed. However, no abnormality is seen in between the seizures in idiopathic epilepsy. Postictal focal signs indicate the focal origin of the seizure.
Figure 9: Signs and symptoms of seizures/epilepsy (Source: www.slideshare.net)
-
Imaging
MRI is indicated especially if the patients experience focal seizures, have focal manifestations or EEG shows focal disturbance. Some of the clinicians run MRI for all the patients with new-onset seizure disorder. CT scan is less sensitive for small abnormalities in brain as compared to MRI. However, CT scan can be considered where MRI is contraindicated e.g. implanted metallic devices. Imaging should be considered in the patients with clinically progressive disorder or in those who develop epilepsy after 20 years of age to rule out space occupying lesion.

Figure 10: MRI for epilepsy (Source: www.alabamanewscenter.com)
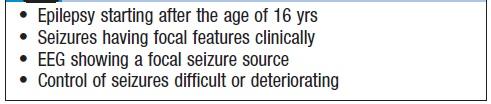
Figure 11: Indications of brain imaging in epilepsy (Walker, et al. 2014)
-
Laboratory and other studies
Initial investigations should include the following:
-
Complete blood count
-
Serum glucose
-
Electrolytes
-
Creatinine
-
Calcium
-
Magnesium
Lumber puncture – if signs of infection are present.
Electroencephalography (EEG) – supports clinical diagnosis, helps determining the prognosis and classifying the seizure disorder. EEG shows paroxysmal abnormalities containing spikes and waves. Classification of seizure disorder is critical to decide the treatment regimen. For example, if absence and focal seizures accompany altered consciousness, it becomes difficult to differentiate between them. Therefore, EEG findings are obtained to differentiate between the types of seizures.
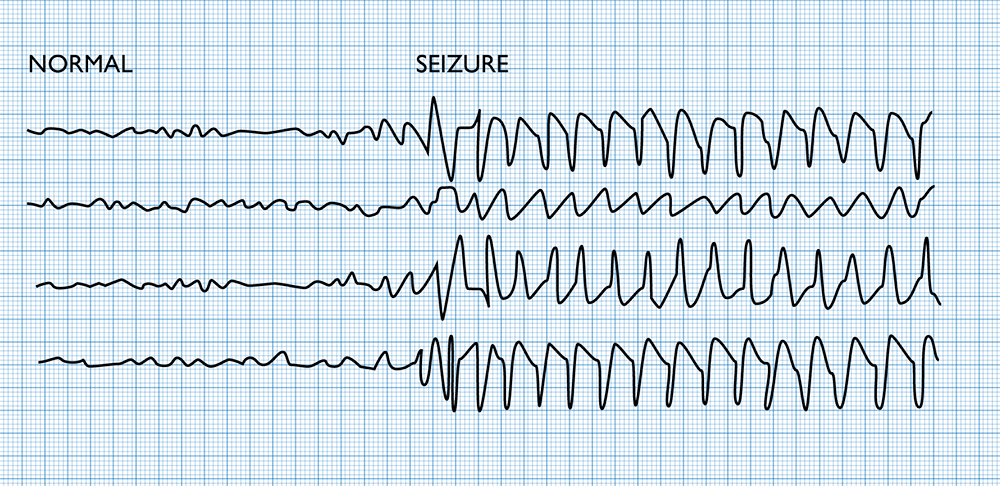
Figure 12: EEG illustration of normal and abnormal brain activity (Source: www.rrapid.leeds.ac.uk)
DIFFERENTIAL DIAGNOSIS
The history of seizures may be similar to various diseases, which may manifest with seizures. Therefore, clear history and supporting investigations help make a diagnosis. There are certain differential diagnoses of seizures which should be kept I mind while dealing with a patient with seizures.
Differential Diagnosis of Focal Seizures
-
Transient ischemic attack – This can be distinguished from a seizure by its longer duration and lack of spread and symptoms.
-
Rage attacks – These are situational and goal-directed.
-
Panic attacks – These attacks have anxiety element and clear relationship with external stimulus.
Differential Diagnosis of Generalized Seizures
Syncope – These attacks are usually associated with postural change, emotional stress, pain or instrumental procedures along with preceding pallor, sweating and nausea. It leads to loss of conscious, which recovers rapidly without any postictal headache or confusion.
Cardiac disease – Cerebral hypoperfusion due to cardiac cause altered consciousness in those who are having cardiac or vascular ailment and present with episodic loss of consciousness. In such patients, no prodromal symptoms are observed. Findings on cardiac auscultation may support the cardiac cause of altered consciousness.
Brainstem ischemia – Brainstem ischemia may also present with loss of consciousness.
Psychogenic non-epileptic seizures (PNES) – These are associated with emotional stress, asynchronous thrashing of limbs and have no postictal behavioral changes. Serum levels of prolactin and creatinine kinase are raised in convulsions but not in PNES.
TREATMENT
-
General Measures
-
Choice of Medication
-
Monitoring
-
Discontinuance of Medication
-
Surgical Treatment
-
Vagal Nerve Stimulation
-
Special Circumstances
-
Solitary Seizures
-
Alcohol Withdrawal Seizures
-
Tonic-Clonic Status Epilepticus
-
Non-Convulsive Status Epilepticus
-
General Measures
The goal of the treatment of the patients with epilepsy or seizures disorder is to avoid further attacks until the patient is seizure-free for at least two years (Papadakis & McPhee, 2015). The patients with epilepsy should be advised to avoid life-threatening or dangerous conditions. Additionally, the doctor should report government authorities about the patient with epilepsy in order to follow legislation such as driving cessation for six months.
Choice of medication
The selection of a drug treatment for the patient with epilepsy depends on the type of seizure. Initially, a single drug should be started and increased gradually until the patient is seizure-free and the side effects of the drug do not prevent further increment in the dose. If the seizures continue despite the maximal doe of the first drug, a second drug is added. The second drug is gradually increased and first drug is gradually withdrawn. The success rate of partial seizures is higher with the following drugs:
-
Carbamazepine
-
Phenytoin
-
Valproic acid
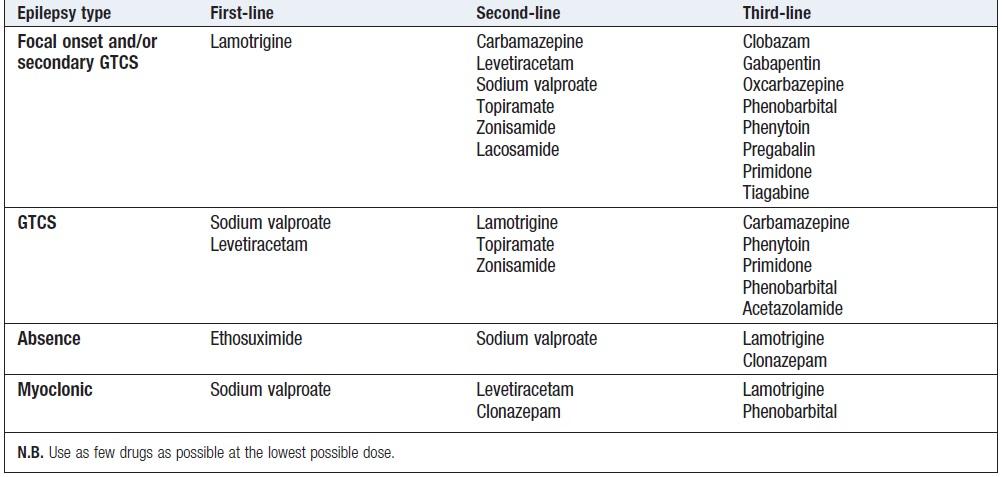
Figure 13: Guidelines for choice of anti-epileptic drug (Walker, et al. 2014)
The other newer drugs used for focal seizures include:
-
Gabapentin
-
Topiramate
-
Lamotrigine
-
Oxcarbazepine
-
Levetiracetam
-
Zonisamide
-
Lacosamide
-
Ezogabine
-
Vigabatrin
-
Tiagabine
Felbamate is used only in selective cases due to its severe side effects like aplastic anemia and fulminant hepatic failure (Papadakis & McPhee, 2015).
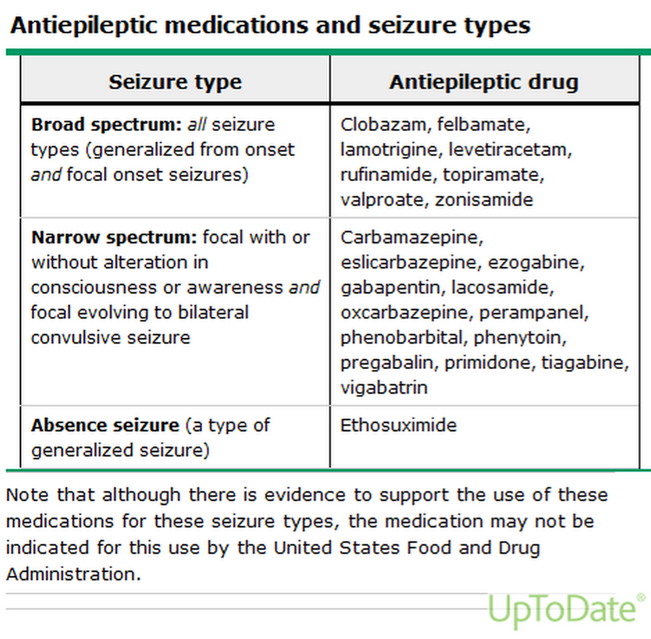
Figure 14: Antiepileptic drugs with seizures type (Source: www.shakenbutnotstirred.weebly.com)
For generalized seizures, valproate is superior to topiramate and lamotrigine. However, its teratogenic effects discourage its use in a pregnant lady. Although all antiepileptic drugs are teratogenic, but antiepileptic drug must be given to prevent seizures as seizures can cause serious adverse effect on the fetus due to trauma, hypoxia and various other factors.
Generally, epilepsy of one type is controlled by a single antiepilelptic drug. However, two drug reduce the frequency of seizures but at increased cost of side effects. Most often, treatment with more than two drugs is unhelpful.
Monitoring
Monitoring of serum drug levels is one of the new advances in epileptic therapy. However, a given dose of a drug produces different serum concentrations and effect because of differences in individual metabolism. Usually, the dose of an antiepileptic drug is increased on the basis of the body’s response. When the target is achieved (seizures are stopped), drug levels are checked for future reference. Compliance of the drug can be increased by decreasing the number of daily doses. However, status epilepticus may occur if the drug is taken erratically.
Laboratory monitoring is required with the use of certain drugs:
-
Periodic liver function tests (LFTs) for valproic acid, carbamazepine, felbamate
-
Serial blood counts for carbamazepine, ethosuxamide, felbamate
Discontinuance of medication
The drug is discontinued if the patient is seizure free for at least two years. Unfortunately, there is no way to predict whether a patient needs a medication or not. The chance of seizures recurrence is more likely in those did not respond to the drug initially, those who have focal signs or those with multiple types of seizures. One drug is withdrawn gradually at one time. If the seizures recur, the most effective drug is started.
Surgical treatment
The patients refractory to drug therapy are the candidates for surgical treatment. Surgical resection is effective if the patient has single well-defined focus.
Vagal nerve stimulation
The patients who show refractory response to drug therapy or are not the candidates for surgery, vagal nerve stimulation is approved for them.
Specific Circumstances
Solitary seizures – It refers to a single solitary attack. In such cases, the underlying cause must be evaluated. EEG should be performed within 24 hours of the attack in order to reach the cause of solitary seizure, especially when focal signs are present. In solitary seizures, prophylactic antiepileptic drug is not needed until further attacks are not observed. Remember, do not diagnose epilepsy on the basis of solitary seizure.
Alcohol withdrawal seizures – Tonic-clonic seizure pattern may be observed in alcohol withdrawal, usually within 24 hours of withdrawal from alcohol. If the seizures show focal features, structural abnormality should be ruled out. CT or MRI brain should be obtained in the patient with new onset generalized fits or those with focal involvement. Anti-convulsant is not required as these are self-limited. Benzodiazepines are effective for the management of seizures caused by alcohol withdrawal.
Tonic-clonic status epilepticus – These seizures are caused by poor compliance with anti-convulsant agents. Such disorders are usually caused by alcohol withdrawal, intracranial infection, tumour, drug intoxication or metabolic disorders. Prognosis of tonic-clonic status epilepticus depends on the period between the initiation and start of effective treatment.
Non-convulsive status epilepticus – Status epilepticus may present with fluctuating abnormal mental status, altered consciousness, confusion, and automatism. EEG established the diagnosis.
REFERENCES
Bromfield EB, Cavazos JE, Sirven JI. (2006) An introduction to epilepsy. West Hartford (CT): American Epilepsy Society. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2511/.
Engel, J.Jr. and Pedley, T.A., eds. (2008) Epilepsy: A Comprehensive Textbook. New York: Cambridge University Press, Lippincott Williams and Wilkins, pp. 2885–2889.
George, A.L.Jr. (2004) Inherited channelopathies associated with epilepsy. Epilepsy Currents, 4(2), 65–70.
Murray, C.J.L., Vos, T., Lozano, R., et al. (2010) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet, 380, 2197–2223.
Papadakis, M.A., McPhee, S.J. (2015) Current medical diagnosis & treatment. New York: McGraw Hill Education.
Santhosh, N.S., Sinha, S. and Satishchandra, P. (2014) Epilepsy: Indian perspective. Annals of Indian Academy of Neurology, 17(Suppl 1), S3–S11.
Walker, B.R., Colledge, N.R., Ralston, S.H. and Penman, I.D. (2014) Davidson’s principles & practice of medicine. 22nd edition. New Delhi: Elsevier, pp. 1179.
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!