Rheumatoid Arthritis
Rheumatoid Arthritis
Course Description
Rheumatoid arthritis (RA) is a disease which affects joints and surrounding tissues [3]. It may affect other organs like the eyes, heart and lungs. It can develop at any age, but usually develops after 35 in women. The onset of the disease during childhood is less frequent. Juvenile RA is a type of disease in which usually manifest before 16 years of age. The severity of the disease increases when it develops in people of younger ages. The main focus of this course is RA in adults.
At the end of this course, the student will be able to know the main causes, pathophysiology and clinical aspects of the disease, treatment of disease and about the extra-articular manifestations.
Accreditation Information: KLA Education Services LLC is accredited by the State of California Board of Registered Nursing, Provider # CEP16145.
Course Certification: Once you have completed this course, click on the “Print Certificate” option below to save or print your CE course certification. If you are not yet registered in a course plan with IvyLeagueNurse, please complete the registration and payment process so that you are able to log into your account and fully obtain your course certificate. Our affordable and unlimited one-year CEU plan starts at just $19.99.
Print Certificate Print Course
Course Objectives
Upon completion of this course, the course participant will be able to:
- Define Rheumatoid Arthritis.
- Describe epidemiology and cost related to rheumatoid arthritis (RA).
- Describe pathophysiology and etiology of RA.
- Identify the clinical signs and symptoms of RA and describe the differential diagnosis.
- Describe the classification of RA.
- Describe the treatment plan of RA.
- Describe the extra-articular manifestations of RA.
Course Content
Epidemiology and Costs

Figure 1: Rheumatoid arthritis (Source www.umm.edu.com)
It is estimated that about 1.5 million adults in America are suffering from RA [1]. The yearly incidence rate of RA is 53 per 100,000 women and it is approximately 27.7 per 100,000 men [1]. The data varies according to different age groups. The incidence rate increases with increasing age of the person in both sexes. The peak incidence is between the ages of 65 to 74 years [1]. In all age groups, women have greater incidence rate as compared to men.
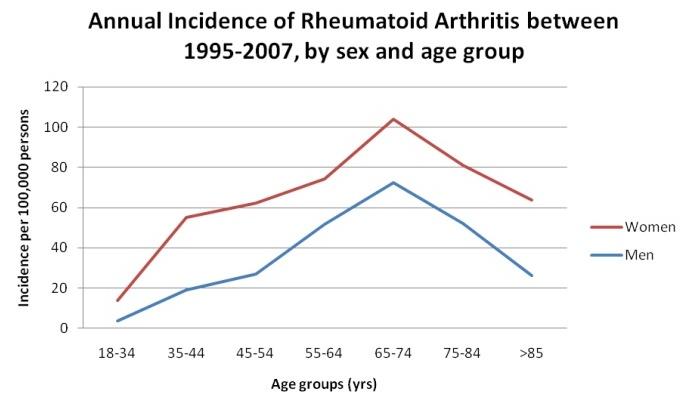
Figure 2: Incidence of RA between 1995-2007, by sex and age group (source: www.prezi.com)
The impact of RA and related arthritic diseases is significantly enough to cause disability and premature mortality in the United States. Many people with RA can do work full-time but some people with RA are so severely affected that they cannot perform the majority of their daily simple activities. The life expectancy of the patient with RA decreases about 3 to 7 years. In severe cases, 10 to 15 years of life from normal life expectancy may be lost.

Figure 3: Disability due to Rheumatoid Arthritis (Source: www.medicinenet.com)
The cost associated with RA is significantly high and is continuously increasing day by day [5]. In 2003, a total of 128 billion dollars were spent for the management of arthritis and other associated rheumatic conditions. About 47 billion dollars were the earning loses from the total cost of 128 billion dollars. Due to RA, many people change their jobs, decrease working hours and even lose the jobs. Smokers have increased risk to develop RA as compared to nonsmokers. Major depression is an associated factor of RA playing a role in developing functional limitation. Mortality rate is higher among the patients with RA as compared to the general population and about one-third to one-half deaths are due to cardiovascular conditions.

Figure 4: Cost of Rheumatoid Arthritis treatment (Source: www.zazzle.com)
Pathophysiology and Etiology
RA is a condition in which chronic inflammatory changes occur in the joints with inflammation of the synovium and cartilage and loss of bone [2]. The exact etiology of RA is currently not known. Usually, it is an autoimmune disease in which autoantibodies (RA factor, anti-citrullinated protein antibody) are produced against the synovial tissues due to misconception of immune system in recognizing the normal synovial tissue as foreign substance [6].
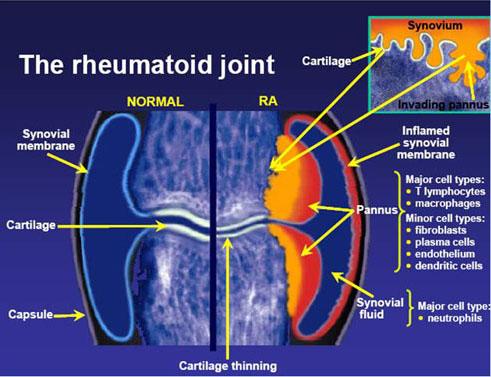
Figure 5: Pathogenesis of Rheumatoid Arthritis (Source: www.mays3.weebly.com)
There are variations present in the course and severity of the illness. Infection, genetic factors and hormones are the contributing factors to the disease. Genetic and environmental factors make a complex interaction with the immune system and synovial tissues to develop RA. Bacteria (Mycobacteria, E. coli, H. pylori, mycoplasma), viruses (Rubella, parvovirus) and superantigents are the triggers to develop RA. Genetically, RA is developed only 1 in 25 white individuals due to shared epitope. If RA is developed in one monozygotic twin, the chance to develop the same disease is 1 in 6.
Figure 6: Etiology of RA (Source: www.medscape.org)
RA develops in joints after passing through many stages. These stages are mentioned below:
-
Synovitis
-
Pannus formation
-
Fibrous ankylosis
-
Bony ankylosis
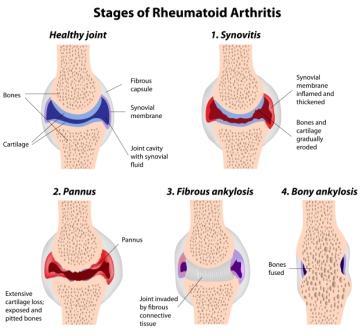
Figure 7: Stages of Rheumatoid Arthritis (Source: www.clinic-hq.co.uk)
Signs, Symptoms and Diagnosis
Presenting Signs and Symptoms
To diagnose RA, a history and physical examination of the patient are very important [7]. Low grade fever and mildly high pulse rate are two findings on general physical examination, otherwise all examination is normal. The characteristic presentation of RA patient is complaining of pain and stiffness in multiple joints [4]. Morning stiffness more than 1 hour is chief complaint of the patient that initiates with fatigue, muscular spasm, weakness and anorexia (loss of appetite).

Figure 8: Symptoms of Rheumatoid Shoulder Joint (Source: www.epainassist.com)
When there is no mobility in the joint for some duration, it inflames and tenderness and stiffness may be experienced by the patient. Due to inflammation, production of synovial fluid is increased and swelling appears on the joint. Accompanying soft tissues are also swollen and joint pain is felt bilaterally all over the body. At resting condition, pain may not be felt in the small joints of hands and feet. Increased blood flow is identified by the palmar erythema and visible veins on the dorsal surface of hand and wrist. Elevated temperature over the involved joint (except hip joint) is felt but no erythema is present. Movement, strength of muscles and function around involved joint are limited.

Figure 9: Rheumatoid Hand (Source: www.gponline.com)
There are rheumatoid nodules (soft, delicate subcutaneous nodules) in the extensor side of the forearm, epitrochlear, axillary and cervical areas may have small soft lymph nodes. Anemia, eye burning and pleurisy (inflammation of lungs) may be present. There may be joint destruction within 1 to 2 years after the onset of the disease.
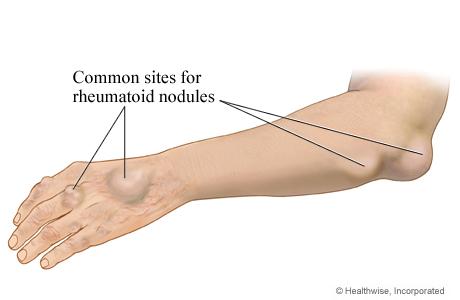
Figure 10: Rheumatoid Nodules (Source: www.webmd.com)
Laboratory Investigations and Imaging
For the diagnosis of RA, many laboratory tests are recommended by The American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR). These tests include:
-
Rheumatoid factor
-
Erythrocyte sedimentation rate (ESR) ≥30 mm/hr
-
C-reactive protein (CRP) ≥0.7 pg/mL
-
Anti-cyclic citrullinated peptide antibody
Rheumatoid factor: The most sensitive and specific laboratory test for RA is positive rheumatoid factor because 70% to 80% of patients have positive rheumatoid factor. It is also present many other conditions mentioned below:
-
Other rheumatic conditions
-
Individuals with chronic infections
-
Many healthy individuals
Anti-CCP antibody: It is a very specific test as it is conducted to confirm the diagnosis of RA. To distinguish RA from other types of arthritis, specific blood test should be carried out. It may be positive in many other diseases like active tuberculosis and early synovitis.
If rheumatoid factor, anti-CCP antibody or subcutaneous nodules are present in an individual, it indicates that he/she is having a severe form of RA.
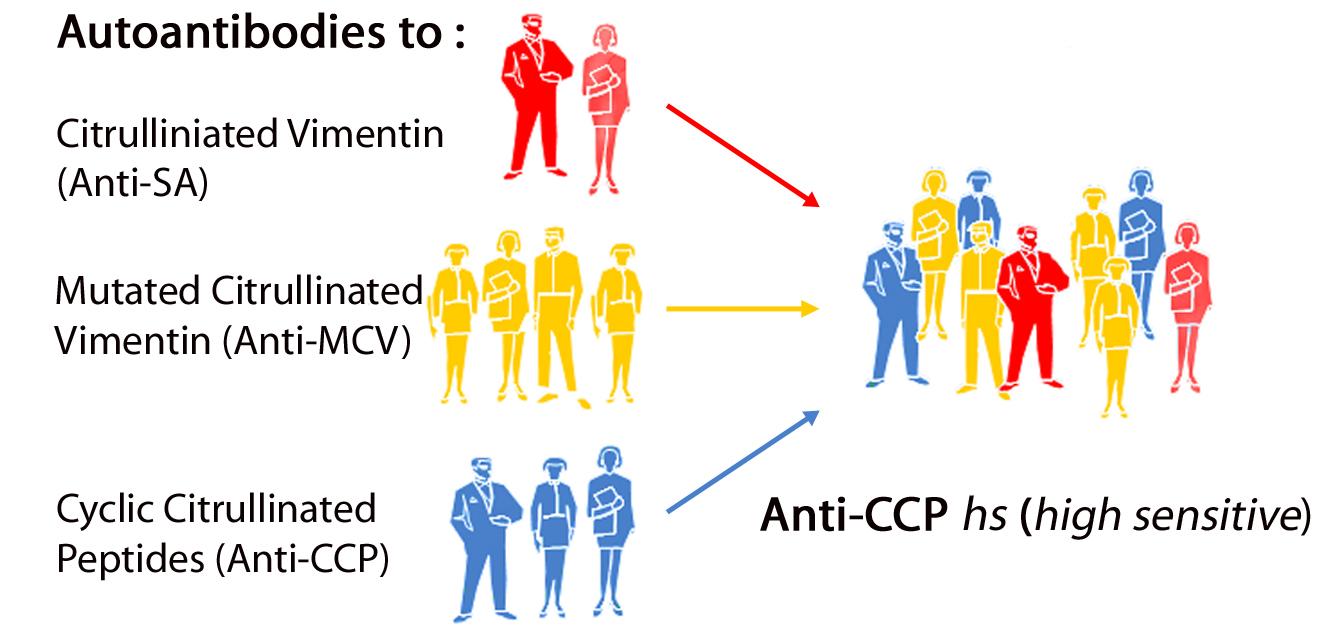
Figure 11: Diagnosis of RA (Source: www.autoimmunityblog.com)
Biomarkers: It is noted that RA is diagnosed on a clinical basis. Biomarkers to diagnose RA have no prognostic accuracy and are insufficient as separate tests, but they are very helpful to find out other causes of arthritis when the clinical features of RA are present in a patient. Vectra DA (a multi-biomarker disease activity test) provides a composite score (1 to 100) by using a unique algorithm. This composite score is made by the results of 12 blood protein biomarkers. These biomarkers are mentioned below:
-
Vascular cell adhesion molecule-1
-
Epidermal growth factor
-
Vascular endothelial growth factor A
-
Interleukin-6 (IL-6)
-
Tumor necrosis factor (TNF) receptor type 1
-
Matrix metalloproteinase-1
-
Matrix metalloproteinase-3
-
YKL-40
-
Leptin
-
Resistin
-
Serum amyloid
-
C-reactive protein (CRP)
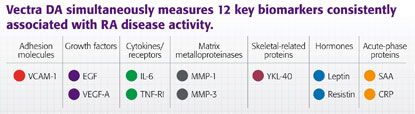
Figure 12: Vectra DA Test (Source: www.vectrada.com)
Routine Baseline Investigations: Many other laboratory tests are performed for the differential diagnosis of RA. In complete blood count, normochromic and microcytic anemia and thrombocytosis may be present. Renal and hepatic function blood tests have no role in the diagnosis of RA; however, these tests are conducted for medication choices.
Arthrocentesis: Sometimes arthrocentesis may be performed by clinicians for the differentiation of RA from other arthropathies. Following findings in the aspirated synovial fluid are in the favor of diagnosis of RA:
-
a lot of fibrin flecks in straw-colored fluid
-
ability of synovial fluid to be clotted at room temperature
-
5,000 to 25,000 WBCs/mm3
-
about 85% polymorphonuclear leukocytes
-
negative bacterial cultures
-
no crystal formations
-
low glucose level

Figure 13: Athrocentesis (Source: www.healthgrades.com)
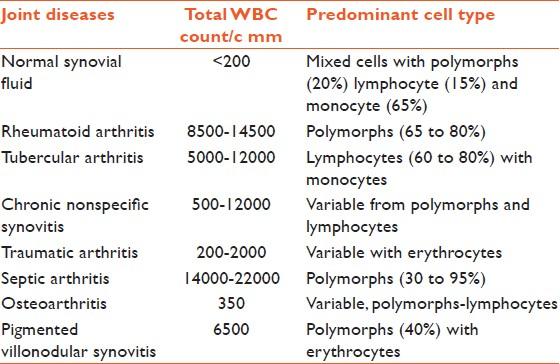
Figure 14: Synovial Fluid Analysis in Normal and Diseased Joints (Source: www.ijabmr.org)
Radiological Investigations: Joint ultrasound, magnetic resonance imaging (MRI) and joint x-rays are most common imaging tests used for evaluation of RA. Following findings may be shown in imaging studies:
-
normal imaging studies
-
osteopenia
-
erosions around joint spaces in early stage of disease
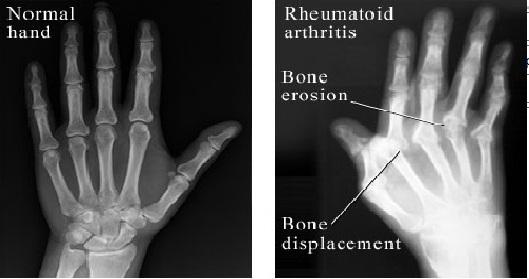
Figure 15: X-ray of RA Hand (Source: myhealth.alberta.ca)
For the implementation of modern treatment strategy in RA, methods are required in which disease is diagnosed at early stage and sensitive monitoring is done during disease process.
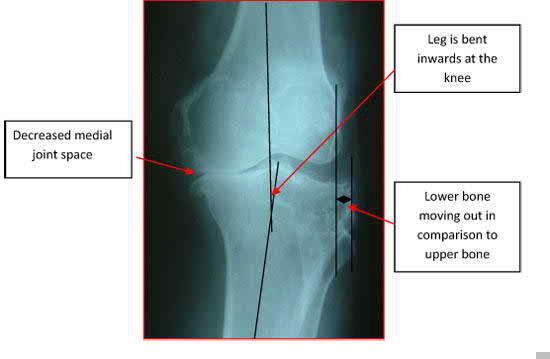
Figure 16: X-ray of Knee Joint showing RA (Source: www.maurascollege.org)
Conventional radiography is usually used to diagnose and monitor structural joint destruction in routine management of RA. Though, bone destruction at early stages and synovitis are not picked up by this conventional radiography. As compared to radiography, early pathology of bone destruction and joint structural changes are better assessed by MRI. MRI can exhibit synovitis in joints without the presence of symptoms. Moreover, changes found in soft tissues including synovitis and tenosynovitis can be assessed in detail by MRI. To get the long term radiological outcomes, findings of MRI are of prognostic importance. Ultrasonography is useful to get information about changes (inflammatory and destructive) appeared in RA finger and toe joints.

Figure 17: Arthritis Knee MRI (source: www.galleryhip.com)
Early detection of joint damage, assessment of inflammatory changes in synovial fluid and curative management of RA patients have been increased significantly by MRI and ultrsonography. It is important for the clinicians to know the MRI and sonography findings of early RA occurring in small synovial joints. Sonography provides a way to identify synovitis and MRI offers a complex approach to pick abnormalities found in small synovial joints.
Diffferential Diagnosis
A lot of medical conditions can be considered as differential diagnosis of RA. These conditions are mentioned in the given table.
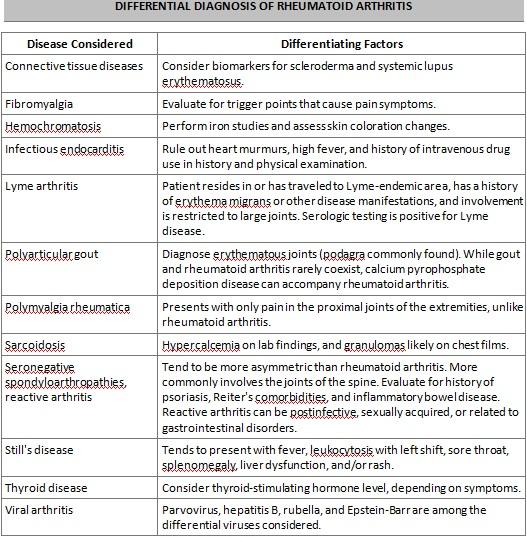
Table 1: Differential Diagnosis of RA
Classification
The classification criteria of rheumatoid arthritis were published by the ACR/EULAR in 2010. 1987 ACR criteria were replaced by these criteria and are taken as standard to classify RA. The new measures mentioned in these criteria have efficient statistical power for the identification of early disease as compared to 1987 response measures. These criteria are mentioned in the given table.
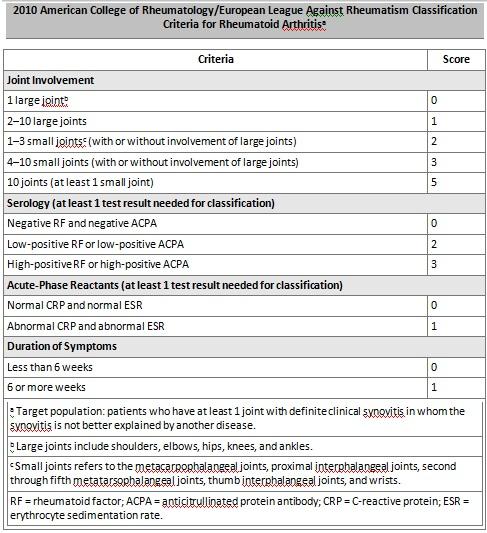
Table 2: Classification Criteria of RA
A patient is declared as having definite RA if the minimum score is 6 points from the established classification system. The concept of classic or probable RA is not present in this system. The global functional report of status is also developed by ACR is given below in table:
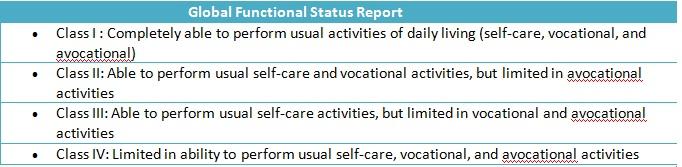
Table 3: Global Functional Status Report
Proposals have been given by the ACR to revise and updated classification scales are provided.
Treatment Options
The treatment for RA is life-long. Medicines, physical exercise and possible surgery are included in the treatment of RA. To get the best results in proper management of RA, the education of the patient is essential. Joint destruction can be delayed by early and aggressive treatment of RA if the diagnosis of RA is made in time. According to the 2010 ACR/EULAR Classification Criteria for Rheumatoid Arthritis, it is recommended immediately after the diagnosis of RA, treatment should be started with disease-modifying anti-rheumatic drugs (DMARDs).
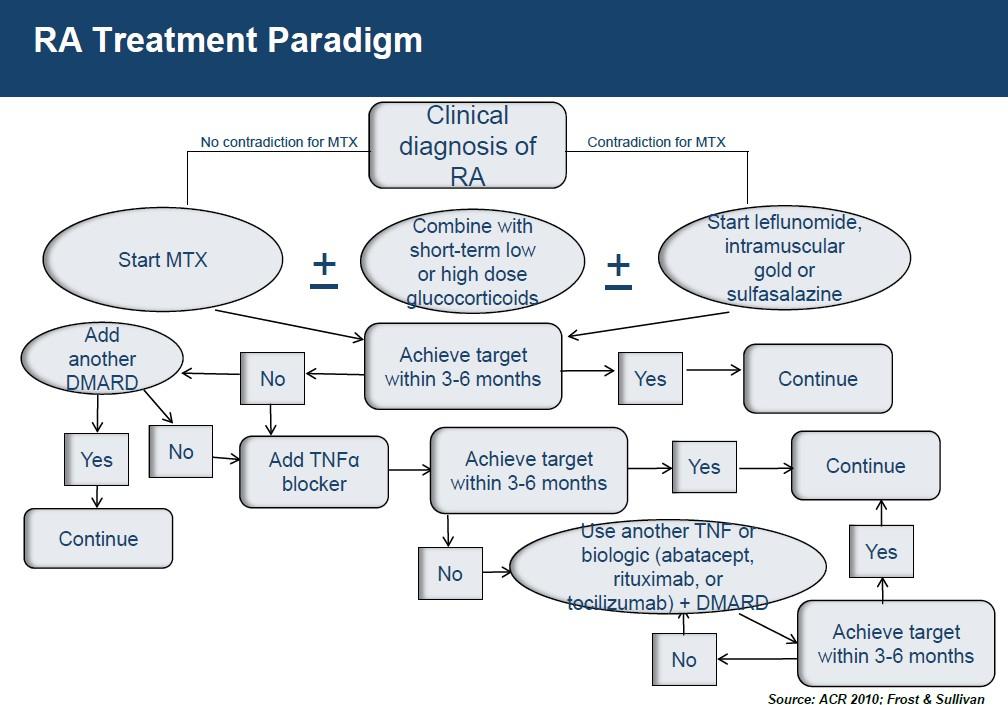
Figure 18: RA Treatment Paradigm (Source: www.frost.com)
Therapeutic goals of treatment are mentioned below:
-
Preservation of function
-
To increase the quality of life
-
To decrease the intensity of pain and inflammation
-
Protection of joint
-
To overcome the systemic complications
-
To minimize the disease activity
-
To avoid from recurrence
Figure 19: Treatment Considerations in RA (Source: www.medscape.org)
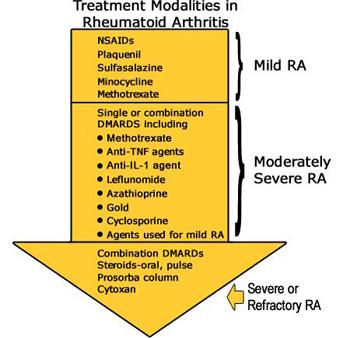
Figure 20: Treatment Modalities in RA (www.hss.edu)
Until the 1980s, “pyramid” approach was used to treat RA pharmacologically. In this approach, treatment was started after diagnosis to alleviate symptoms. If the symptoms enhanced or aggravated, dose of the medicine was modified and more medicines were included. Non-steroidal anti-inflammatory drugs were started first to alleviate the pain. If this treatment was ineffective, DMARDs were started later on. In new research, DMARD, especially methotrexate, is initiated after diagnosing RA [15]. In severe cases, NSAIDs, oral or intra-articular low dose glucocorticoids are added to the treatment for the control of symptoms.
Figure 21: 1980s Approach to Traet RA (Source: www.medscape.org)
Now-a-days, it is recommended standard in treatment to focus on each patient to get a specific target (reduction or minimum disease activity) in specified time frame (normally 6 months) by modifying the medication regimen for individual [11]. In the “treat-to-target” approach, methotrexate (DMARD) is initiated immediately after diagnosis in a patient with high disease activity and features of poor prognosis. Quick improvement and decreased progress in joint destruction are achieved by initiating combination therapies with DMARDs in those patients who are presented with high disease activity. Few adjustments are needed in treatment to withdraw combination therapies successfully as compared to monotherapies. Strict monitoring (every one to three months) is needed in patients with active disease. If the patient does not show improvement in the first three months, treatment adjustment should be made. DMARD monotherapy is typically started in those patients who have low to moderate disease activity or have highly active disease but poor prognostics features are not present.

Figure 22: Changes in the Treatment of RA (Source: www.medscape.org)
Disease Modifying Anti-rheumatic Drugs
Currently, the standard pharmaceutical care of RA is DMARDs. Several factors are seen to choose DMARD as treatment for a patient. These factors are mentioned below:
-
compliance of the patient
-
severity of the disease
-
clinical experience of the physician
-
various comorbidities present in the patient
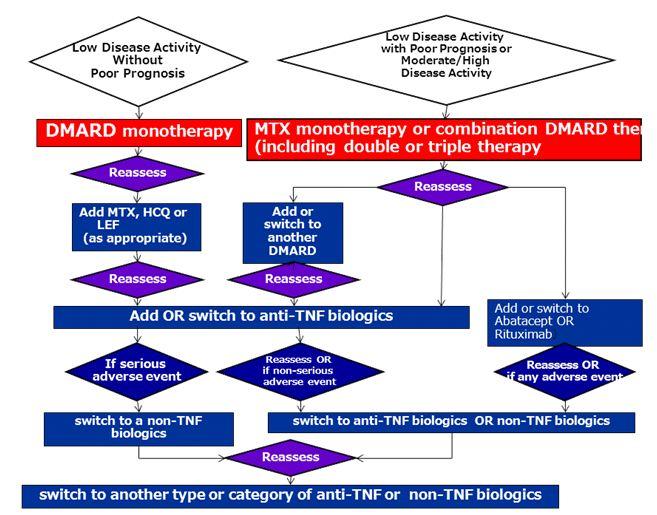
Figure 23: DMARDs (Source: www.intechopen.com)
Most commonly used DMARDs are listed in a table below. Common adverse effects are also mentioned in the table.
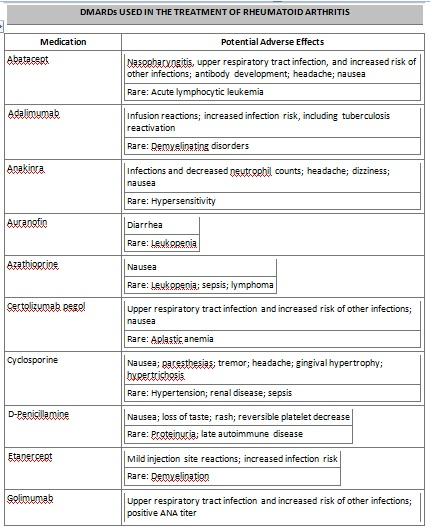
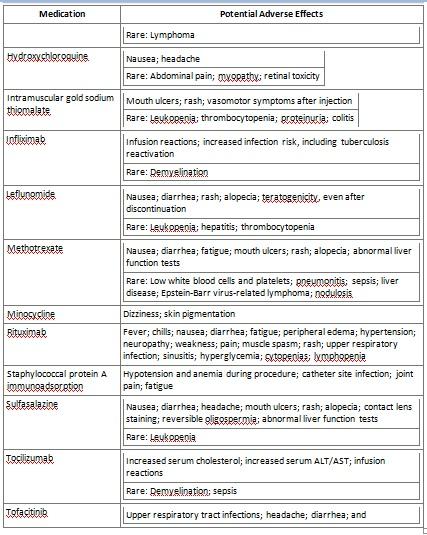

Table 4 : Disease Modifying Anti-Rheumatic Drugs
Methotrexate is a DMARD that is prescribed most commonly and known as “anchor drug” for treating RA [14]. Leflunomide is a newer DMARD with good efficacy and can be used as substitute therapy in those patients who cannot tolerate methotrexate or methotrexate is contraindicated. To add leflunomide with methotrexate may be beneficial in those patients who are not responding to methotrexate monotherapy. Other commonly used DMARDs are listed below:
-
Hydroxychloroquine
-
Minocycline
-
Sulfasalazine
-
Anti-TNF biologic agents
-
-
Adalimumab
-
Etanercept
-
Infliximab
-
Certolizumab pegol
-
Golimumab
-
-
Non-TNF biologic agents
-
Abatacept
-
Anakinra
-
Rituximab
-
Tocilizumab
-
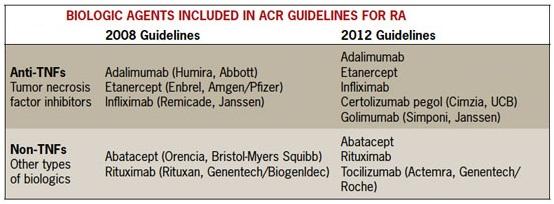
Figure 24: Biological Agents (Source: www.hcplive.com)
Sulfasalazine and hydroxychloroquine are used in treatment of malaria but these drugs are commonly prescribed to treat RA as first-line treatment [14]. Weeks or months are required to get effect from the anti-malarial medications. Two or three DMARDs are combined commonly and are used as first-line treatment in those cases where disease activity is moderate or high and poor prognostic features are present.
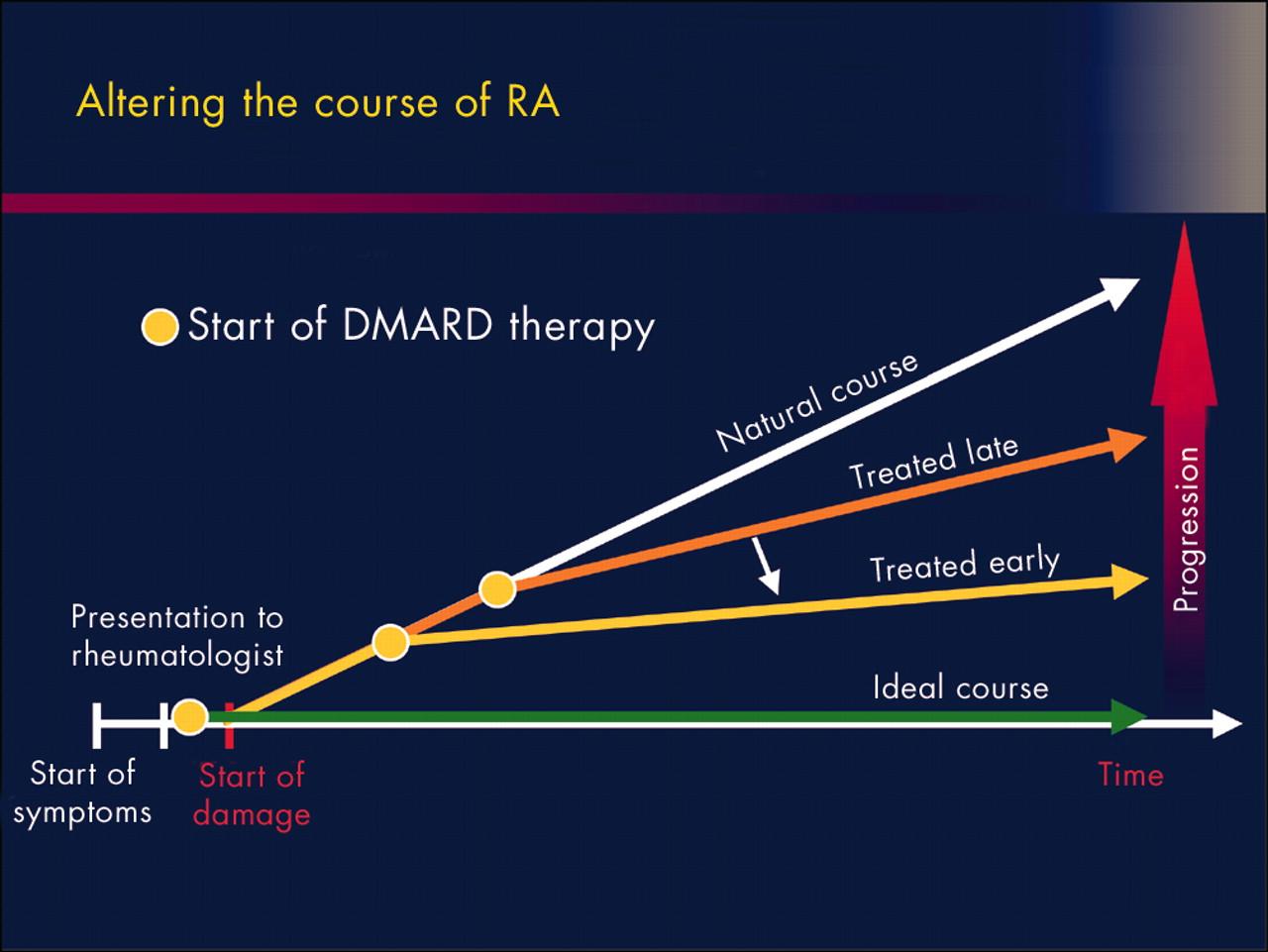
Figure 25: DMARD Therapy (Source: www.idhumanbody.com)
Biological agents: These are considered as well known drugs in DMARD therapy [13]. Non-TNF agents are only prescribed when disease is not responding to TNF-alpha inhibitors or any contraindications are there for TNF-alpha inhibitors. TNF-alpha inhibitors decrease the inflammation process by inhibiting the proteins causing inflammation. These agents are given to patients by subcutaneous or intravenous route. By the action of these agents, raised TNF-alpha levels in synovial fluid of RA patients are lowered. Anemia due to RA is also improved by treatment of these agents.
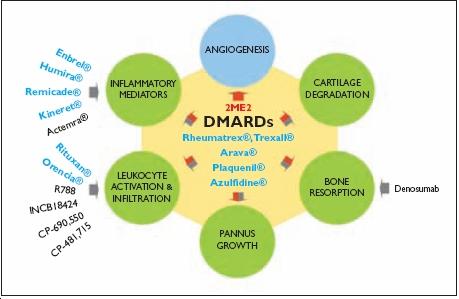
Figure 26: DMARDs (Source: ddw.net-genie.co.uk)
Etanercept (souble TNF alpha receptor blocking agent) provides long term effects of treatment as compared to methotrexate and symptoms are rapidly improved.
Infliximab provides a greater response in those patients who are not responding to methotrexate [17].
An additive effect is received when Adalimumab is given with methotrexate [10].
Certolizumab Pegol is a specialized anti-TNF agent in which conjugation is made between an antigen binding fragment (Fab’) from a monoclonal antibody and polyethylene glycol [8]. It is given to patients by subcutaneous route. Due to its unique structure, some cytotoxic side effects appeared due to other anti-TNF agents are not shown. It can be prescribed to pregnant women because it cannot cross the placenta.
The non-TNF agents control the inflammatory process by modulating specific white blood cells. Abatacept acts on T cells and decreases their count and in response to decreased T cells, other cells involved in inflammatory process are not activated.
Anakinra blocks the interleukin-1 (IL-1) receptor and provides more results when given as monotherapy or combination therapy with methotrexate. It has ability to decrease joint space erosions and osteoporosis due to RA. Many adverse effects are associated with the use of Anakinra. These adverse effects are mentioned below:
-
irritation of skin at the site of injection
-
increased infection risk
-
leucopenia
Rituximab is an antibody that acts on the B-cell surface receptor and decreases abnormally produced B-cells in RA patients. It is administered twice a year by intravenous route.
Tocilizumab is inhibitor of IL-6 receptor and prevents the cytokine to activate the immune response. It is given per month in the form of IV infusion. The safety of this agent is similar to other non-TNF biologic agents.
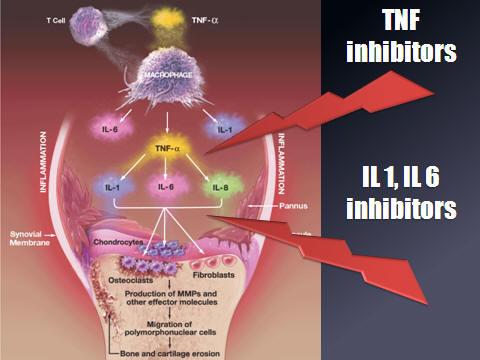
Figure 27: Mechanism of Action of Biologic Agents (Source: www.arthritis.co.za)
Tofacitinib acts by inhibiting the Janus kinase receptor and is taken orally [16]. The recommended dose is 5 mg two times a day, but the dose can be reduced to 5 mg once daily when renal and hepatic functions are moderately reduced. Some warnings mentioned below should be kept in mind while using this agent:
-
risk for serious infection
-
tuberculosis
-
lymphoma
-
other malignancies
Anti-Inflammatory Medications
NSAIDs, glucocorticoids and cyclooxygenase-2 (COX-2) inhibitors are considered as anti-inflammatory drugs and are commonly used to get relief from joint pain and inflammation due to RA [9]. These drugs have no role in the alteration of disease course and should not be prescribed as monotherapy.
Serious adverse effects are associated with these medications. Following complications are associated with the long term use of NSAIDs:
-
gastrointestinal bleeding
-
myocardial infarction
-
stroke
-
gastric ulcer
COX-2 Inhibitors inhibit the action of cyclooxygenase (an enzyme that promotes inflammation). These agents were working initially as traditional NSAIDs with minimum side effects. Reports of stroke and myocardial infarction due to use of these agents have narrowed the wide range of these drugs.
Figure 28: Traditional Treatment Pyramid for RA (Source: www.medscape.org)
Joint swelling and inflammation is decreased by the use of corticosteroids and it is very effective and safe intervention to treat single joint temporarily by injecting glucocorticoid. Infectious arthritis is a contra-indication for intra-articular injections. RA symptoms can be relieved as well as joint damage can be slowed down by the daily steroid dosage of lower than 10mg of prednisone. Due to potential long term adverse effects, corticosteroids should be administered for minimum time at the minimum possible doses. Side effects are mentioned below:
-
osteoporosis
-
cataract
-
cushing syndrome
-
blood glucose level problems
It is recommended by ACR that calcium (1,200-1,500mg) and vitamin D (800-1,000 IU) should be taken daily by the patients on corticosteroid therapy to avoid corticosteroid induced osteoporosis. When the steroid therapy is discontinued, symptoms may recur especially when treated with high dosage. So, withdrawal of agents should be tapered off to avoid rebound symptoms. When DMARDs are started, system steroids work as “bridging therapy” up to that time when effectiveness of DMARD appears.

Figure 29: Conventional Medications for RA (Source: www.slideshare.net)
Sometimes, it is needed to perform surgery for the correction of severely affected joints. The surgeries performed on the knees and hips are mostly successful. Synovectomy is the first surgery that is done in which joint lining (synovium) is separated. Temporary relief is obtained from this procedure, but it is more effective in those patients in whom no improvement is obtained from the pharmacologic treatment. Total joint replacement with a joint prosthesis is done in the patients in whom the onset of the disease is in old age. Surgeries are performed to get following mentioned benefits:
-
to relieve joint pain
-
to correct deformities
-
to improve joint functions
Physiotherapy
Physiotherapy is performed to postpone the loss of joint function [18]. For the support and alignment of joints, some therapists apply heat and cold treatments and splints or orthotic devices. For the reduction of pain and improvement in joint mobility, specialized devices are used by some therapists for the application of deep heat or electrical stimulation. Occupational therapies improve the disabilities by constructing splints for hands and wrists. They encourage the patients with RA to manage the limitations in a better way.

Figure 30: Physiotherapy for RA (Source: www.aplusphysio.co.nz)
Lifestyle Interventions
Along with medical management, numerous lifestyle changes in RA patients are helpful in improving severity of the symptoms and reduction in the number of break-outs. Recommended lifestyle changes are mentioned below:
-
rest and exercise
-
use of orthotic devices
-
stress reduction
-
healthy diet
Exercise
Exercise is advised by the primary care providers to improve general health and RA related symptoms. Low intensity exercises are recommended to enhance the strength of function [19]. More intense exercises may enhance the symptoms of RA and destruction of affected joints. Generally following benefits can be obtained by performing exercises:
-
Improvement in intensity of pain
-
Betterment in the upper limb and lower limb force
-
Improvement in functional status
-
Overall function enhancement
-
Reduction in number of sick days

Figure 31: Exercise for RA (Source: www.6minutes.com.au)
Orthotic Devices
Splints are helpful in some patients of RA while using for short period of time. These devices are used to get following benefits:
-
rest of the effected joint
-
support of the effected joint
-
stabilization of affected joint

Figure 32: RA: Orthotic Device (Source: www.newhopepando.com)
Stress
Stress enhances the RA associated proinflammatory load leading towards the more severe disease. The cellular production of IL-6 is greatly stimulated in the RA patients due to chronic interpersonal stress. Stressful events enhance the symptoms of RA in already stressed patients. Few interventions are designed to decrease the stress and develop the skills to cope stressful events. These are mentioned below:
-
biofeedback
-
breathing techniques
-
meditation
-
yoga
-
mindfulness
Extra Articular Manifestations
In RA, only joint is not destructed, almost all the body organs can be involved [12]. Some extra articular manifestions of RA are given in the following table.
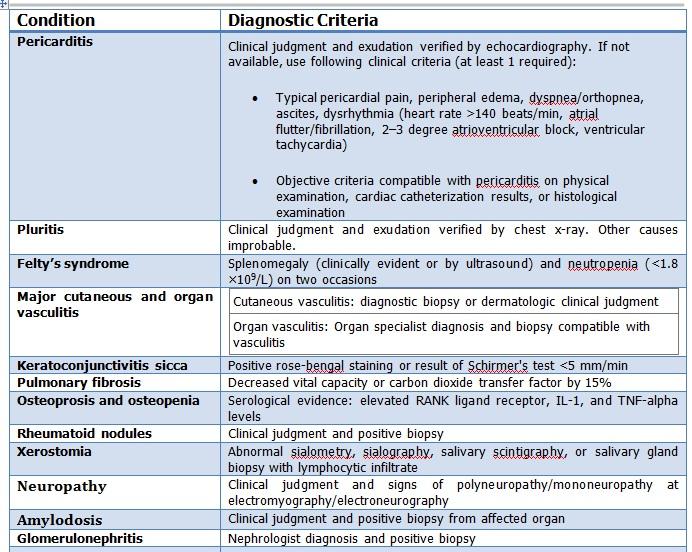
Table 5: Extra Articular Manifestations of RA
Cardiovascular Manifestations
Congestive cardiac failure may occur due to the RA because pericarditis (inflammation of cardiac outer covering) and myocarditis (inflammation of cardiac muscle) may be developed due to RA [20]. Risk for the development of cardiovascular disease is more in the people with RA as compared to those who are without RA.
Unrecognized myocardial infarction (MI) and sudden cardiac death are more common in patients of RA because angina symptoms are not developed in these patients. The physical activity is decreased and body mass index is also low due to RA. There are more chances to develop hypertension, diabetes and high cholesterol level in the patients of RA as compared to those without RA.
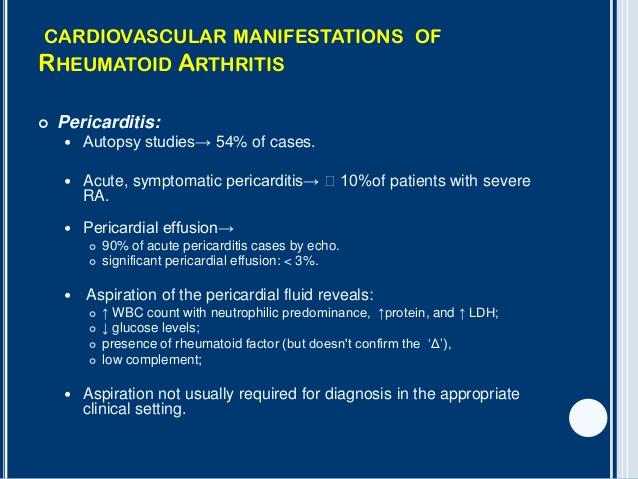
Figure 33: Cardiovascular manifestations of RA (Source: www.slideshare.net)
Pulmonary Manifestations
RA patients may also develop pulmonary manifestations [21, 22].
Common pulmonary manifestations are mentioned below:
-
Pleural effusion
-
pulmonary rheumatoid nodules
-
interstitial pneumonitis
-
pulmonary fibrosis
Pleuritis is usually identified during autopies of RA patients. Most often, the patients present with dyspnea because pleural effusion is developed enough to cause dyspnea. Pleuratic pain is not the chief complaint of the patient. Pulmonary inflammatory disease may be the cause of development of pulmonary fibrosis.
In early stages of interstitial lung disease, pulmonary mononuclear cell infiltrate is developed in patients with RA; later on pulmonary fibrosis is developed as the interstitial lung disease progresses. Smoking is the major risk factor to develop fibrotic complications in the lungs of the patients with RA as compared to other patients in general population.
Figure 34: Pulmonary manifestations in RA (Source: www.medscape.com)
Vasculitis
Inflammatory vascular diseases that are developed in the patients of RA are grouped under the term “vasculitis” [23, 24]. Firstly, inflammation develops in the medium and small sized blood vessels. Stroke or heart failure may be developed in these patients due to involvement of the brain, nerves and heart by development of infections or neuropathy. The incidence of rheumatoid vasculitis is marked decreased due to noticeable betterment in therapy due to excessive utilization of methotrexate and new biologic drugs. Levels of rheumatoid factor and manifestation of vasculitis are strongly associated with RA. Immune complexes containing rheumatoid factor and immunoglobulin produced due to vascular damage are deposited intravascularly.
Ocular Involvement
Following mentioned manifestations are due to ocular involvement in RA patients:
-
scleritis
-
anterior uveitis
-
peripheral ulcerative keratitis
Due to ocular mononuclear cell infiltrates, inflammatory cytokines are produced in these disorders. In keratoconjuntivitis sicca, dryness is developed in both cornea and conjunctiva. Levels of rheumatoid factor and keratoconjunctivitis have association with RA.
Figure 35: Ocular Manifestations of RA (Source: www.slideshare.net)
Osteopenia and Osteoprosis
Osteopenia and osteoporosis are commonly manifested in patients with RA. There is no association between the development of osteopenia and corticosteroid therapy in patients with RA. Osteoclastic bone resorption is promoted due to increased levels of RANK ligand expressed by T cells. Infammatory markers and osteopenia in RA are directly associated. RANK ligand production is augmented due to high levels of IL-1 and TNF-alpha produced in inflamed synovium of RA.

Figure 36: X-ray of RA patient: osteopenia (Source: www.oftankonyv.reak.bme.hu)
Anemia
Most of the patients with RA develop hematologic abnormalities, especially anemia [25]. Increased levels of inflammatory cytokines (TNF-alpha, IL-1, and IL-6) cause the anemia of chronic disease in RA patients.
Rheumatoid Nodules
Rheumatoid nodules are commonly present in the patients of RA. The most common position of these nodules is subcutaneous tissue in pressure areas (elbow and finger joints). These nodules may be developed in internal organs (pleura, lungs, larynx and meninges) of the body [26].
In mature rheumatoid nodule, collagenous capsule covers the central area of necrosis surrounded by palisading fibroblast and chronic inflammatory cells surround the capsule. Activation of complement system and terminal vasculitis due to affected small arterioles are the source of development of nodule. Due to proliferation of resident histiocytes and macrophages influx from the circulation, immunological response is mediated.
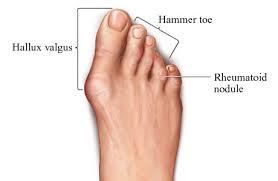
Figure 37: Rheumatoid Nodule (Source: www.natura2000communicationplatform.eu)
Figure 38: Extra-articular Changes in RA (Source: www.slideshare.net)
Cervical Spine Instability
Due to degeneration of ligaments and bone in the cervical spine, instability of cervical spine is commonly manifested in patients of RA [27]. Due to this inherent instability, neuropathy can be developed due to minor trauma. Careful examination is needed in patients with RA after road traffic accidents, minor falls and other traumas to rule out cervical spine injury. Commonest symptom after cervical spine injury is the pain radiation towards occiput. Slow progressive quadriparesis along with loss of sensations in the hands is less common with cervical spine injury.
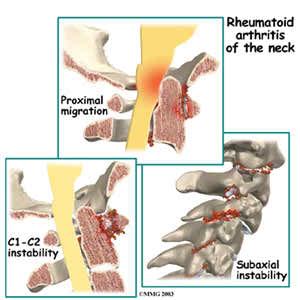
Figure 39: Rheumatoid Arthritis of the neck (Source: www.stephenessesmd.com)
Conclusion
RA is a devastating disease which affects the daily activities of the patients due to inflammation of joint cavities and the overall quality of life is affected. Health care professionals should know the common symptoms and signs of the disease to avoid the early diagnose. The management of disease requires proper diagnostic modalities. This disease has many extra-articular manifestations like cardiovascular involvement, pulmonary fibrosis, interstitial lung disease, vasculitis, ocular involvement and cervical spine instability etc. They should know the new emerging treatments of this disease.
Symptoms are relieved in some patients by the standard therapies but some patients show resistance to the therapy and emerging therapies are used to treat the disease. The effective management of RA is beneficial for both the health care providers and patients.
References
-
Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising? Results from Olmsted County, Minnesota, 1955–2007. Arthritis Rheum. 2010;62(6):1576-1582.
-
Cooles FA, Isaacs JD. Pathophysiology of rheumatoid arthritis. Curr Opin Rheumatol. 2011;23(3):233-40.
-
Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010 Sep 25;376(9746):1094-108.
-
Smith HS, Smith AR, Seidner P. Painful rheumatoid arthritis. Pain Physician. 2011 Sep-Oct;14(5):E427-58.
-
Kobelt G, Jönsson L, Lindgren P, Young A, Eberhardt K. Modeling the progression of rheumatoid arthritis: a two-country model to estimate costs and consequences of rheumatoid arthritis. Arthritis Rheum. 2002;46(9):2310-9.
-
Klareskog L, Stolt P, Lundberg K, Källberg H, Bengtsson C, Grunewald J, et al. A new model for an etiology of rheumatoid arthritis: smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to modified by citrullination. Arthritis Rheum. 2006;54(1):38-46.
-
Kung TN, Bykerk autoantigens VP. Detecting the earliest signs of rheumatoid arthritis: symptoms and examination. Rheum Dis Clin North Am. 2014 Nov;40(4):669-83.
-
Keystone EC, Curtis JR, Fleischmann RM, Furst DE, Khanna D, Smolen JS, et al. Rapid improvement in the signs and symptoms of rheumatoid arthritis following certolizumab pegol treatment predicts better longterm outcomes: post-hoc analysis of a randomized controlled trial. J Rheumatol. 2011;38(6):990-6.
-
Haus E, Sackett-Lundeen L, Smolensky MH. Rheumatoid arthritis: circadian rhythms in disease activity, signs and symptoms, and rationale for chronotherapy with corticosteroids and other medications. Bull NYU Hosp Jt Dis. 2012;70(1):3-10.
-
Rau R, Simianer S, van Riel PL, van de Putte LB, Krüger K, Schattenkirchner M, et al. Rapid alleviation of signs and symptoms of rheumatoid arthritis with intravenous or subcutaneous administration of adalimumab in combination with methotrexate. Scand J Rheumatol. 2004;33(3):145-53.
-
Heidari B. Rheumatoid Arthritis: Early diagnosis and treatment outcomes Caspian J Intern Med. 2011;2(1):161–170.
-
Cojocaru M, Mihaela-Cojocaru I, Silosi I, Doina-Vrabie C, and Tanasescu R. Extra-articular Manifestations in Rheumatoid Arthritis Maedica (Buchar). 2010;5(4):286–291.
-
Taylor PC, Feldmann M. Anti-TNF biologic agents: still the therapy of choice for rheumatoid arthritis. Nat Rev Rheumatol. 2009;5(10):578-82.
-
O'Dell JR, Haire CE, Erikson N, Drymalski W, Palmer W, Eckhoff PJ, et al. Treatment of rheumatoid arthritis with methotrexate alone, sulfasalazine and hydroxychloroquine, or a combination of all three medications. N Engl J Med. 1996;334(20):1287-91.
-
Suarez-Almazor ME, Belseck E, Shea B, Wells G, Tugwell P. Methotrexate for rheumatoid arthritis. Cochrane Database Syst Rev. 2000;(2):957.
-
Lee EB, Fleischmann R, Hall S, Wilkinson B, Bradley JD, Gruben D, et al. Tofacitinib versus methotrexate in rheumatoid arthritis. N Engl J Med. 2014;370(25):2377-86.
-
St Clair EW, van der Heijde DM, Smolen JS, Maini RN, Bathon JM, Emery P, et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: a randomized, controlled trial. Arthritis Rheum. 2004;50(11):3432-43.
-
Hurkmans EJ, van der Giesen FJ, Bloo H, Boonman DC, van der Esch M, Fluit M, et al. Physiotherapy in rheumatoid arthritis: development of a practice guideline. Acta Reumatol Port. 2011;36(2):146-58.
-
Balsamo S, Diniz LR, dos Santos-Neto LL, da Mota LM. Exercise and fatigue in rheumatoid arthritis. Isr Med Assoc J. 2014;16(1):57-60.
-
Ortega-Hernandez OD, Pineda-Tamayo R, Pardo AL, Rojas-Villarraga A, Anaya JM. Cardiovascular disease is associated with extra-articular manifestations in patients with rheumatoid arthritis. Clin Rheumatol. 2009;28(7):767-75.
-
Gauhar UA, Gaffo AL, Alarcón GS. Pulmonary manifestations of rheumatoid arthritis. Semin Respir Crit Care Med. 2007;28(4):430-40.
-
Antin-Ozerkis D, Evans J, Rubinowitz A, Homer RJ, Matthay RA. Pulmonary manifestations of rheumatoid arthritis. Clin Chest Med. 2010;31(3):451-78.
-
Turesson C, Matteson EL. Vasculitis in rheumatoid arthritis. Curr Opin Rheumatol. 2009;21(1):35-40.
-
Vollertsen RS, Conn DL. Vasculitis associated with rheumatoid arthritis. Rheum Dis Clin North Am. 1990;16(2):445-61.
-
Baer AN, Dessypris EN, Krantz SB. The pathogenesis of anemia in rheumatoid arthritis: a clinical and laboratory analysis. Semin Arthritis Rheum. 1990;19(4):209-23.
-
Kitamura A, Matsuno T, Narita M, Shimokata K, Yamashita Y, Mori N. Rheumatoid arthritis with diffuse pulmonary rheumatoid nodules. Pathol Int. 2004;54(10):798-802.
-
da Côrte FC, Neves N. Cervical spine instability in rheumatoid arthritis. Eur J Orthop Surg Traumatol. 2014 Jul;24 Suppl 1:S83-91.
Course Exam
Before you receive your certificate, you must complete the exam and achieve a score of % or higher. (You have unlimted attempts).
This exam is required by your state licensure.
Exam
Exam
We are required to delay the exam hours. Check back soon!
Exam
We are required to delay the exam until you have had time to view the course material. Please view the course first!
No Licenses on File
Please add a license to your account before you continue. Thank you!